
Lung Cancer
- BONUS Official
- May 7, 2024
- 1 min read
Updated: May 9, 2024
Lung cancer is one of the most common cancers and the leading cause of cancer death worldwide.

Definition"A group of malignant epithelial tumours arising from cells lining the lower respiratory tract." [1]
EpidemiologyIn 2018, a total of 47,838 people were diagnosed with lung cancer with 35,137 deaths recorded in the United Kingdom
This represents 13% of all new cancer diagnoses, making it the 3rd most common cancer.
Lung cancer is the most common cause of death due to malignancy, accounting 21% of all cancer deaths
1-year survival is 83% for patients with stage 1 and 17% for stage 4 disease.
References: [2], [3]
Risk Factors / CausesUp to 79% of lung cancer in the United Kingdom are preventable [3].
Causes include:
Tobacco (73%) - smoking 72%, environmental exposure 1%
Occupation (13%) - asbestos (8%), other materials such as silica, diesel engine exhaust, TCDD, radon, mineral olds, arsenic welders, and paint (1%)
Air pollution (8%)
Ionising radiation (5%)

Anatomy / PathophysiologyLung cancer can be divided into two pathological classifications [4]:
Small cell lung cancer (SCLC) represents about 20% of all lung cancers
Non-small cell lung cancer (NSCLC) represents about 80% of all lung cancers
Small cell lung cancer
Highly aggressive neuroendocrine malignancy
Most strongly associated with smoking relative to other subtypes
Arise centrally with mediastinal involvement
Often presents with metastatic disease at the time of diagnosis
Commonly associated with paraneoplastic syndromes
Non-small cell lung cancer
NSCLC can be subdivided into three subtypes:
Adenocarcinoma
40% of all lung cancers
Most common type of lung cancer in non-smokers
Arise from mucous-secreting glands (pneumocytes or club cells) in the alveolar or bronchiolar epithelium of peripheral airways
Histologically characterised by the presence of glandular differentiation and/or mucin production
Squamous cell carcinoma (SCC)
20% of all lung cancers
Arise from the bronchial epithelium of large, central airways
Progresses from preinvasive neoplastic lesions: squamous metaplasia, squamous dysplasia, or carcinoma in situ
The majority are centrally located, arising from segmental bronchi
Histologically characterised by intercellular bridges, keratinisation and squamous pearl formation
Large cell carcinoma (LCC)
3% of all lung cancers
Diagnosis of exclusion, where the tumour does not demonstrate any morphological features of adenocarcinoma, SCC or SCLC
Poorly differentiated, partially necrotic tumours
Signs and SymptomsSigns:
Localised dullness to percussion
Wheeze, crackles and/or decreased breath sounds
Cervical or supraclavicular lymphadenopathy
Finger clubbing
Symptoms:
New or persistent cough
Dyspnoea
Haemoptysis
Chest or shoulder pain
Weight loss
Hoarseness (secondary to paralysis of the recurrent laryngeal nerve)
Dysphagia (obstruction of oesophagus)
Confusion, personality changes, seizures, headache, nausea or vomiting (brain metastasis)
Bony pain, pathological fractures (bone metastasis)
Facial swelling, dilated neck or chest/abdominal wall veins (superior vena cava syndrome)
Paraneoplastic syndromes:
Hypercalcaemia of malignancy, most commonly due to ectopic parathyroid hormone release causing hypercalcaemia (most commonly seen in SCC)
Syndrome of inappropriate antidiuretic hormone production (SIADH) causing hyponatraemia (most commonly seen in SCLC)
Ectopic Cushing's syndrome (ECS) through ectopic production of ACTH (most commonly seen in SCLC)
Hypertrophic osteoarthropathy causing painful symmetrical arthropathy (SCLC only)
Lambert-Eaton myasthenic syndrome (LEMS) causing proximal muscle weakness (almost exclusively seen in SCLC)
References: [1], [5], [6]
InvestigationsChest x-ray
Contrast-enhanced CT of the lower neck, thorax and upper abdomen
Other possible investigations:
CT PET and CT/MRI head if considering treatment with curative intent
If a pleural effusion is present, consider a diagnostic thoracentesis
If suitable for invasive investigations, consider bronchoscopy +/- endobronchial ultrasound (EBUS) with brushings, washings and alveolar lavage or transbronchial needle aspiration biopsy
Mediastinal lymph node biopsy using mediastinoscopy and endobronchial ultrasound (EBUS)
Any biopsy should be tested for mutations in:
EGFR
ALK
ROS1
PD-L1
BRAF
NTRK
C-MET
RET
KRAS
HER2
References: [1], [6], [7]
Staging / GradingThe TNM staging system is a universal standard for classifying the extent of cancer. There are 3 components for this system [8].
Tumour (T): size and extent of the primary tumour
Node (N): regional lymph node involvement
Metastasis (M): presence of metastatic spread
As the TNM staging system is updated regularly, we recommend you stick to the version that your hospital uses. You can find the information about the TNM staging system version 8.0 here: 10.1634/theoncologist.2017-0659
ManagementFor non-small cell lung cancer (NSCLC):
Stage I-IIA
If suitable for treatment with curative intent, lobectomy (open or thoracoscopic) is usually offered with hilar and mediastinal lymph node sampling.
If surgery is declined or contraindicated, radical radiotherapy (SABR, stereotactic ablative radiotherapy) or sub-lobar resection can be offered.
Stage II and III
Offer multimodality treatment if suitable (a combination of surgery, radiotherapy and/or chemotherapy).
Consider chemoradiotherapy if surgery is declined or contraindicated.
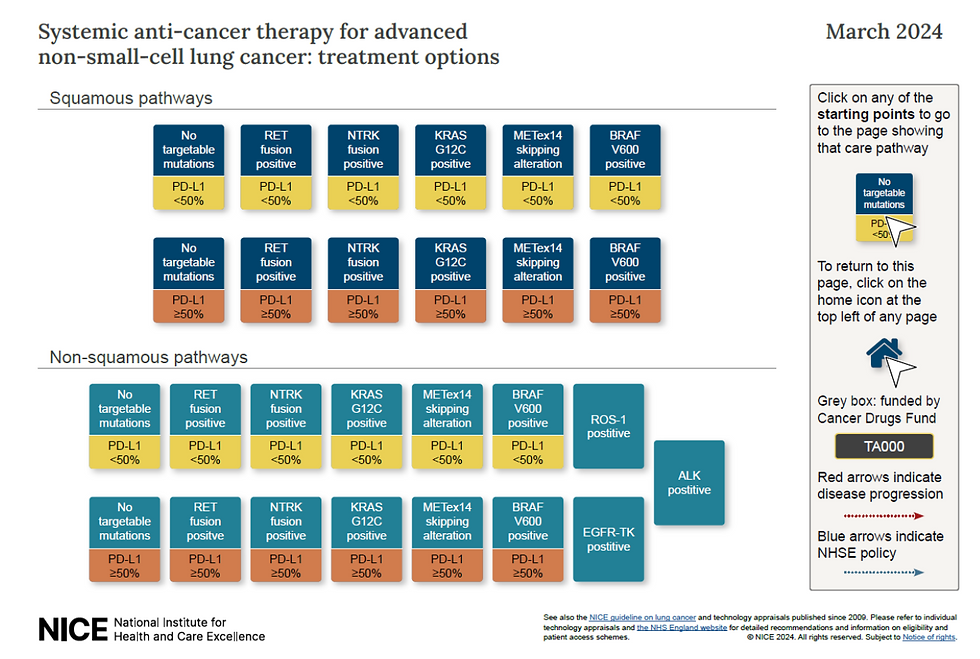
Stage IV
Systemic anti-cancer therapy: platinum doublet chemotherapy, immunotherapy, or targeted therapies.
For small cell lung cancer (SCLC):
Limited stage disease
Surgery may be considered in early-stage SCLC.
4-6 cycles of platinum-based chemotherapy with radiotherapy (either twice-daily or once-daily, or sequential depending on fitness and performance status).
Prophylactic Cranial Irradiation (PCI) should be discussed and considered to prevent possible brain metastasis.
Extensive-stage disease
Platinum-based combination chemotherapy up to a maximum of 6 cycles
Reference: [7]
Referral CriteriaReferral using the suspected cancer pathway (appointment within 2 weeks) if:
CXR findings suggestive of lung cancer
Age > 40 and unexplained haemoptysis
Urgent CXR (performed within 2 weeks) if (1) age > 40 and 2 or more of the following symptoms or (2) have ever smoked or been exposed to asbestos and have 1 of the following symptoms:
Cough
Fatigue
Shortness of breath
Chest pain
Weight loss
Appetite loss
Urgent CXR (performed within 2 weeks) if age > 40 and any of the following:
Persistent or recurrent chest infections
Finger clubbing
Supraclavicular lymphadenopathy or persistent cervical lymphadenopathy
Chest signs consistent with lung cancer or pleural disease
Thrombocytosis
References: [9]
ScreeningNHS Lung Health Check service is offered in some parts of England and Wales for patients:
55 - 74 (60 - 74 in Wales)
Have ever smoked
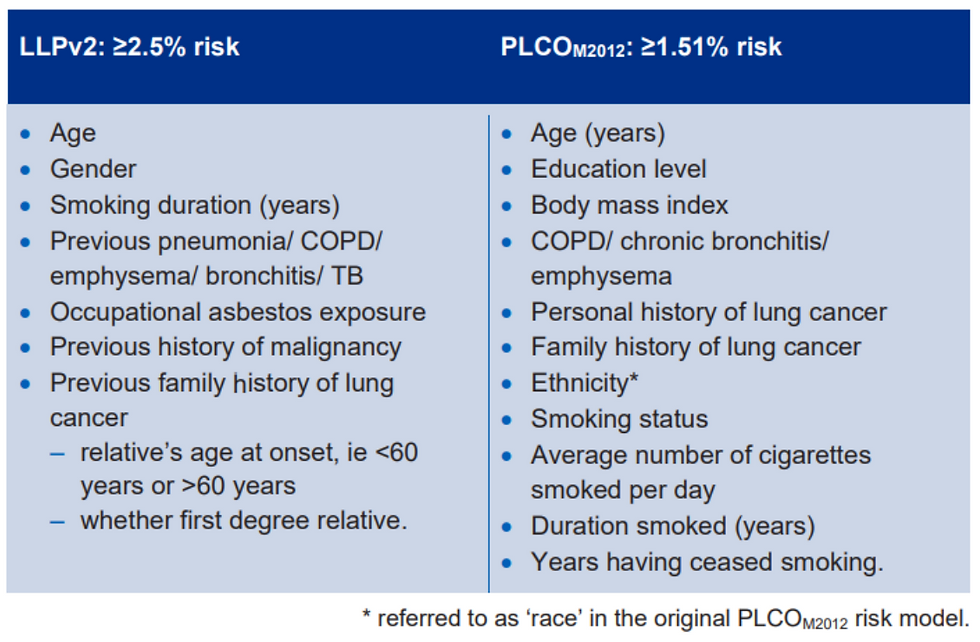
Initial appointment to calculate lung cancer risk using risk prediction models:
If PLCOM2012 risk of ≥ 1.51% over six years or LLPver2 five-year risk of ≥ 2.5% invite for low dose CT-scan (LDCT)
References: [10], [11]
Resources[1] BMJ Best Practice. Non-small cell lung cancer. 2024 [Available from: https://bestpractice.bmj.com/topics/en-gb/1082.
[2] Navani N, Baldwin DR, Edwards JG, Evison M, McDonald F, Nicholson AG, et al. Lung Cancer in the United Kingdom. Journal of Thoracic Oncology. 2022;17(2):186-93.
[3] Cancer Research UK. Lung cancer statistics. 2024 [Available from: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/lung-cancer.
[4] Davidson MR, Gazdar AF, Clarke BE. The pivotal role of pathology in the management of lung cancer. J Thorac Dis. 2013;5 Suppl 5(Suppl 5):S463-78.
[5] Spiro SG, Gould MK, Colice GL. Initial Evaluation of the Patient With Lung Cancer: Symptoms, Signs, Laboratory Tests, and Paraneoplastic Syndromes: ACCP Evidenced-Based Clinical Practice Guidelines (2nd Edition). Chest. 2007;132(3, Supplement):149S-60S.
[6] BMJ Best Practice. Small cell lung cancer. 2024 [Available from: https://bestpractice.bmj.com/topics/en-gb/1081.
[7] National Institute for Health and Care Excellence. Lung cancer: diagnosis and management. 2024 [Available from: https://www.nice.org.uk/guidance/ng122.
[8] Detterbeck FC, Boffa DJ, Kim AW, Tanoue LT. The Eighth Edition Lung Cancer Stage Classification. Chest. 2017;151(1):193-203.
[9] National Institute for Health and Care Excellence. Lung and pleural cancers - recognition and referral 2021 [Available from: https://cks.nice.org.uk/topics/lung-pleural-cancers-recognition-referral/.
[10] NHS England. Standard protocol prepared for the Targeted Lung Health Checks Programme 2022 [Available from: https://www.england.nhs.uk/wp-content/uploads/2019/02/B1646-standard-protocol-targeted-lung-health-checks-programme-v2.pdf.
[11] Cancer Research UK. Lung Health Checks 2024 [Available from: https://www.cancerresearchuk.org/about-cancer/lung-cancer/getting-diagnosed/lung-health-checks.
Author: Ilse Trip






Comments